







Uterine Fibroid Embolization (UFE)
Uterine Fibroid Embolization(UFE) is a non-surgical minimally invasive procedure blocking the blood supply to the uterine fibroids, causing them to shrink down, effectively treating fibroid symptoms & avoiding invasive surgical procedures and associated complications.
Performed under local anaesthetic and twilight sedation, UFE is low risk with a quick recovery and 90% patient satisfaction long-term.
UFE QUICK SUMMARY
- Long and heavy periods?
- Pelvic pain?
- Need to pee frequently?
- Bleeding between periods?
- Pain during sex?
- Looks like you’re pregnant?
- Feeling bloated?
- Back pain?
- Want to keep your uterus?
- Fibroids causing infertility?
- Minimally invasive – shrinks ALL the fibroids, by blocking blood supply
- Treats underlying cause and preserves the uterus
- NHS ‘A’ rating for UFE
- Treats all types of fibroids
- Performed under twilight sedation, no general anaesthetic needed
- Short hospital stay – can go home the next day
- A recommended treatment for fibroid-related infertility
UFE: The Full Story
What are uterine fibroids?
Fibroids are non-cancerous growths of muscle and fibrous tissue that arise in the wall of the uterus.
As many as 8 out of 10 women develop fibroids at some point in their life.
Fibroids usually start growing during a woman's reproductive years (from around the age of 16 to 50) when oestrogen levels are at their highest.
There may be just one or two fibroids or sometimes quite a few, up to 9 or 10. The fibroids can be just a few centimetres in size, but some may grow to be quite large, up to 20cm.
They tend to shrink when oestrogen levels are low, such as after the menopause when a woman's monthly periods stop. However, women taking hormone replacement therapy (HRT) which contains oestrogen may find the fibroids become a problem again.
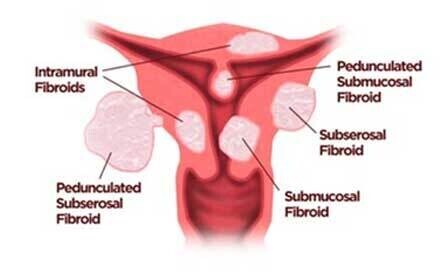
Fibroids grow in different parts of the uterus:
- Intramural - within the uterus wall, these are the most common type
- Subserosal - on the outer surface of the uterus wall
- Submucosal - on the inner surface of the uterus, under the endometrial lining
- Pedunculated - the fibroid is on a stalk, either inside or outside the uterus
Fibroid symptoms
Typical symptoms are:
- heavy and prolonged periods
- bleeding between periods
- pelvic pain
- bloating
- big tummy
- needing to pee frequently
- Constipation
- Back and leg pain
- Pain during sex
- trouble getting pregnant
- repeated miscarriages
Some women with a few fibroids have no symptoms and are unaware they are present.
However, for many women symptoms are common and can be severe.
The symptoms are related to the fibroid size and position within the uterus.
Fibroids in the wall or inside the uterus cause over-activity of the uterus lining, resulting in heavy and prolonged periods, also bleeding between periods.
Fibroids inside the uterus can cause pain or block the fallopian tubes affecting fertility, also they may cause early miscarriages.
Fibroids in the wall and on the outer surface can make the uterus and tummy much bigger, like you are pregnant or just feel bloated. The fibroids also release hormones (prostaglandins) that can cause bloating.
The expanded uterus can press on the bladder causing frequent urination and on the bowel resulting in constipation, also they may press on the vagina making sex uncomfortable.
The fibroids may press on nerves in the back causing back and leg pain.

What is Uterine Fibroid Embolization (UFE)?
Fibroids rely on a continuous supply of blood from the uterine arteries to maintain their size and continue to grow.
UFE is a low-risk minimally invasive non-surgical treatment that blocks the arteries feeding the fibroids with micro-sized particles. By limiting or completely eliminating the fibroids’ blood supply, the fibroids shrink over time and die. All the fibroids are targeted in one treatment whilst preserving normal anatomy of the uterus. In the UK, UFE has been recognised by NICE (National Institute of Clinical Excellence) since 2007 as one of the standard treatments for fibroids.
UFE is performed under local anaesthetic and twilight sedation, so a general anaesthetic is not needed. The whole procedure is performed through a tiny 2mm nick in the skin overlying the right groin or the wrist. Ultrasound and high resolution low-dose real-time X-ray imaging are used to accurately guide the embolization. During UFE, a tiny tube called a microcatheter is manipulated from the skin entry point to the uterine artery on one side within the pelvis.
The safe position of the microcatheter tip within the uterine artery is confirmed by injecting a dye that shows up on X-ray. Following this, tiny particles measuring 300-500 microns in size are carefully infused through the microcatheter. The particles flow with the blood down the uterine artery and block the very small arteries in the fibroids by effectively silting them up.
Once one side is completed, the microcatheter is manipulated to other side and the process repeated to fully treat fibroids on both sides of the uterus. Compared to other fibroid treatments the recovery is quick. You will be in hospital for 1 or 2 nights. On average patients feel back to normal after two and half weeks.
The fibroids take 6-9 months to fully shrink down, however most patients have considerable improvement in their symptoms by 3 months.
What are the advantages of UFE?
- Minimally invasive procedure
- Preserves the uterus
- Treats all the fibroids, reducing chances of recurrence
- Performed under local anaesthetic and twilight sedation
- No general anaesthetic
- No incision or stitches
- Treats all types of fibroids
- Quick recovery – home after 1 or 2 nights, on average back normal after 2.5 weeks
- 90% of patients satisfied or very satisfied at 4 years
- Low risk procedure – allows early treatment when fibroids are easier to control.
- Fertility is preserved and may be improved

Who is suitable for UFE?
UFE is good treatment for all types of fibroids: small or large, single or multiple, also any position within the uterus.
Early treatment of fibroids leads to better long-term results. Because UFE is a lower risk procedure, it can be offered earlier than surgical procedures. Hysterectomy and myomectomy have a longer recovery and higher rate of complications, so tend to be offered when symptoms are more severe.
Fertility After UFE
Having a healthy pregnancy and delivery are both possible after UFE. A 2017 study published in the journal Radiology investigated 359 women with fibroids unable to conceive who then underwent UFE. The researchers of the study followed up after an average of about six years. In that time, 149 women, or 41.5%, became pregnant at least once and 131 women gave birth to a total of 150 babies. It was the first pregnancy for over 85% of these women.
The researchers concluded that UFE can be recommended to women with fibroids as a treatment option that restores fertility.
UFE can also be an effective treatment for adenomyosis.
Women who have recurrent fibroids and symptoms after other treatments such as myomectomy and endometrial ablation are also still suitable for UFE.
What are the alternative treatments?
Hysterectomy (surgical removal of the uterus) has for many years been the main treatment for fibroids and certainly relieves symptoms as all the fibroids are taken out along with the uterus. It is a major operation with 4-6 days in hospital and 2-3 months recovery. The serious complications rate is 4-6% which includes bladder and ureter damage, infection, bleeding, wound dehiscence and chronic problems such as bowel dysfunction, bowel obstruction and vaginal prolapse.
Myomectomy is an operation which removes individual fibroids, it is either done as a ‘key-hole’ procedure or through an incision in the tummy. It has a quicker recovery time and lower complication rate than hysterectomy, however generally not all the fibroids can be removed, so recurrence of symptoms may occur as the remaining fibroids are untreated.
Endometrial Ablation burns the lining of the uterus to treat heavy and prolonged periods. Only the lining of the uterus is treated, it does not reduce the size of the fibroids.
What tests are needed?
It is most likely your GP has already arranged an ultrasound of the pelvis to confirm the presence of fibroids.
We will also arrange an MRI (Magnetic Resonance Image) of pelvis to fully characterise the fibroids and look for any other possible causes of your symptoms.
You will also need to have had a normal cervical smear test within the last 18 months.
In preparation for the UFE you will have some routine blood tests done (clotting, full blood count, urea and electrolytes).
Who will be doing the UFE?
UFE is performed by an Interventional Radiologist (IR).
IRs are trained and certified in minimally invasive image-guided techniques such as embolization. They are also certified in the interpretation of the ultrasound and MRI imaging needed to diagnose fibroids and other problems in the pelvis.
Your UFE will be performed by Dr Nick Burfitt, Interventional Radiology Consultant.
Dr Burfitt became a consultant in 2007 at Imperial College NHS Healthcare Trust, specializing in embolization & IR techniques throughout the body, he has been performing UFE since 2006, seeing patients in both the NHS and private sector.
For more information about Dr Nick Burfitt click here.
Where will the UFE take place?
In the Interventional Radiology Department at The Cromwell Hospital, London
UFE is performed in a dedicated image-guided operating theatre. Whilst Dr Burfitt is performing the UFE, you will be carefully monitored and cared for by the specially trained IR nursing staff.
A Radiographer will also be present to control the imaging equipment.
How do I prepare for my UFE?
Do not eat for 6 hours before the UFE, it is ok to drink clear liquids (water, squash, tea and coffee without milk) up to 2 hours before the procedure.
Please take your regular medications as normal with a sip of water.
What actually happens during UFE?
We will get you comfortable lying on the image-guided operating table.
The nurse looking after you will give you an intravenous sedative and painkillers to keep you comfortable and relaxed. You will also have an intravenous antibiotic to prevent any infection.
Your blood pressure, heart rate and oxygen levels will be monitored closely throughout the procedure.
Depending on the artery access point, the skin over the groin or wrist will be cleaned and sterile drapes placed over you.
Local anaesthetic will be injected through a fine needle under the skin and down to the artery, this will sting a little for about a minute and then go numb.
A small access tube (less than 2.5mm in diameter) will be carefully inserted into the artery under ultrasound guidance, once this is in position you will not really be aware of what is happening inside the arteries.
A very tiny tube called a microcatheter (0.7mm in diameter) is then steered under real-time low-dose X-ray into the uterine artery on one side.
The correct position of the microcatheter tip within the prostate artery will be confirmed by injecting a dye which shows up on X-ray, confirming the exact correct position for the embolization.
Following this, tiny polymer beads measuring 350 to 500 microns in size are carefully infused through the microcatheter. The beads flow with the blood down the uterine artery and block the very small arteries within the fibroids by effectively silting them up.
Once one side is completed, the microcatheter is manipulated to the other side, from the same access point and the process repeated to fully treat both sides of the uterus.
At the end of the UFE all tubes are removed. In the groin a very small collagen plug is placed at the artery access site to help stop any bleeding, your body absorbs the plug over the next few months. At the wrist pressure is applied for about 20 minutes to the artery access site to stop any bleeding.
How long does the UFE take?
Most UFEs take about 45 minutes of actual procedure time, sometimes a bit longer - up to 90 mins, usually when the fibroids are large, or the angles to the uterine arteries are a bit tricky.
Does UFE hurt?
The local anaesthetic at the beginning of the procedure stings a bit for around 60 seconds.
Towards the end of treating the first side, patient usually start to get some pain and cramping in the uterus which is similar to period pain. We give intravenous sedation and opiate painkillers before and throughout the UFE to keep this pain under control.
After the UFE, patients experience pelvic pain for between 8 to 16 hours. This may be mild or quite severe. To keep you comfortable, you will have an intravenous opiate painkiller infusion running which you control by pressing a button (PCA – patient controlled analgesia).
What happens after the UFE?
Once the UFE is completed, you will be transferred back to your private room on the ward for observation and bed rest for 4 hours. You can eat drink normally immediately after the UFE.
You will stay in hospital overnight to keep the pelvic pain under control with the intravenous PCA. Once you no longer need intravenous painkillers, you can go home, usually around lunchtime the next day.
We will send you home with a week’s course of antibiotics and painkillers.
You will have our contact details if there are problems or you want to ask any questions.
The expected side effects after UFE
In the first two weeks after the UFE, most patients have some cramping pains which are controlled with the painkiller tablets provided. You may also have a mild temperature for about a week and feel quite tired – this is called post embolization syndrome and is an expected side effect.
Some vaginal bleeding or brown discharge may occur for a few weeks. Most patients feel ‘back to normal’ at around two and a half weeks.
Arranging two weeks off work is recommended.
In about 5% of cases a submucosal fibroid may detach from the uterine wall, fall into the cavity, and pass out of the vagina. If the fibroid is too large to pass it may require assisted removal by a gynecologist. Fibroid expulsion can occur days to several months after the procedure.
Follow up after the UFE
Dr Burfitt will contact you by telephone 3 weeks after the UFE to see how you are doing.
At 9 months after the UFE, we will arrange an MRI of the pelvis. This will be followed by a clinic appointment with Dr Burfitt to review the outcome of your UFE.
You will have our contact details if there are problems or you want to ask any questions at any time.
The possible complications after UFE
Occasionally there may be some bleeding from the artery access site at the groin or wrist which will cause bruising in the surrounding skin, sometimes a small collection of blood may form called a haematoma. The haematoma generally resolves by itself, but if it became large we would ask you to come back for review.
Although uncommon, infection is the biggest concern following UFE. You should get back in contact with us if you develop a high temperature, a smelly vaginal discharge or the pain is getting worse not better. We may to need to bring you back into hospital and treat you with intravenous antibiotics for a few days. Very occasionally, if the infection gets out of control, then a hysterectomy may be required. However, this is very rare, happening in less than 1% of patients.
Normal periods usually restart at 3-4 months. Very occasionally periods may stop altogether due ovarian failure or early menopause. This is a rare a complication, occurring in less than 0.5% of patients and almost always in patients over 45 years old.
Patients dying following UFE is very rare – less than 1 in 25,000 and is usually because of infection. To put this into perspective, death following hysterectomy is significantly higher at 1 in 1000 to 1,500, this is 16-25 times more common.
UFE history and results
Since the 1970’s embolization of the uterine arteries has been used with excellent life-saving results to treat severe uterine bleeding from cancers, surgery and child birth.
In fibroid patients, at first embolization was done before myomectomy surgery as a method of decreasing the blood loss that occurs during the myomectomy operation, but doctors soon realised that after the embolization, many patient’s symptoms went away and the myomectomy was no longer needed.
After making this discovery, UAE was then used as a treatment specifically for fibroids in France in the early 1990’s. Since that time several 100,000 UFEs have been performed worldwide.
In terms of results, UFE shrinks fibroids by 40% to 75% in the first 6 months, they continue to shrink over longer periods of time. This reduction in fibroid size causes the uterus to shrink by 26% to 59%. Most women get significant symptom relief by three months after the UFE.
A study of 200 women asked about their symptoms 3 months after treatment reported that 87% described improvement in their bleeding symptoms, and 93% described improvement in pelvic pain and pelvic pressure symptoms.
A long term study showed 90% of patients were satisfied or very satisfied at 4 years after UFE.

UFE and pregnancy
Having a healthy pregnancy and delivery are both possible after UFE. A 2017 study published in the journal Radiology investigated 359 women with fibroids unable to conceive who then underwent UFE. The researchers of the study followed up after an average of about six years. In that time, 149 women, or 41.5%, became pregnant at least once and 131 women gave birth to a total of 150 babies. It was the first pregnancy for over 85% of these women.
The researchers concluded that UFE can be recommended to women with fibroids as a treatment option that restores fertility.
Adenomyosis
Adenomyosis is a condition in which cells from the lining of the womb (which sheds and bleeds during a period) are present within the muscle of the womb. It is a progressive condition that causes enlargement of the uterus, heavy periods and pain, also fertility can be affected. Symptoms usually start after the age of 35. Adenomyosis and fibroids may be present together.
Adenomyosis is a difficult condition to treat, traditionally hysterectomy has been performed for severe cases. Mild symptoms maybe improved with the Mirena coil or endometrial ablation.
UFE has been successful in treating adenomyosis, but the results are not as good as for fibroids. UFE significantly improves heavy bleeding and pain in the short to medium term, also with reduction in the size of the uterus by up to 45%. At least 50-80% of women will have continued benefit from UFE after 2 years.
UFE and the Mirena coil maybe used in combination to control adenomyosis symptoms.
Improved fertility and successful pregnancy is also reported following UFE treatment of adenomyosis.
References
Uterine artery embolization for symptomatic uterine fibroids (Review). Cochrane Library. Gupta et al. (2014).
Current evidence on uterine embolization for fibroids. Seminars in Interventional Radiology, [9] Spies, J. B. (2013). 30(4), 340–346
Ruuskanen, A., Hippeläinen, M., Sipola, P., & Manninen, H. (2010). Uterine artery embolisation versus hysterectomy for leiomyomas: Primary and 2-year follow-up results of a randomised prospective clinical trial. European Radiology, 20(10), 2524–2532.
Jun, F., Yamin, L., Xinli, X., Zhe, L., Min, Z., Bo, Z., & Wenli, G. (2012). Uterine artery embolization versus surgery for symptomatic uterine fibroids: A randomized controlled trial and a meta-analysis of the literature. Archives of Gynecology and Obstetrics, 285(5), 1407–1413.
Randomised comparison of uterine artery embolisation (UAE) with surgical treatment in patients with symptomatic uterine fibroids (REST trial): 5-Year results. BJOG: An International Journal of Obstetrics and Gynaecology, Moss, J. et al (2011). 118(8), 936–944.
Magnetic Resonance Imaging (MRI) Analysis of Fibroid Location in Women Achieving Pregnancy After Uterine Artery Embolisation. Walker WJ et al, Cardiovascular interventional Radiology - August 2007
Spontaneous pregnancy with a live birth after conventional and partial uterine fibroid embolization. Radiology, Pisco, J et al. Jun (2017).; 13: 161495.